By Shiena Serikawa
As I write this on my way home from Uganda, I can easily remember the first day of my internship at the Centre of Health, Human Rights and Development (CEHURD). Entering the office extremely nervous, I was surprised that it was half-empty. Later I learned that most of the team was away in the field. This reflects the nature of work at CEHURD which values direct interactions and engagements with communities.
My first day began with a conversation with Jane, one of the lawyers at CEHURD, which I hold dear to my heart to this day. She told me that she strives to fight for the fundamental health and human rights everyone deserves and that the smiles on the faces of community members and the words of thank you after bringing legal services closer to them are more than enough to keep her going. Although my understanding of the work at CEHURD was far from complete at the time, her words inspired me to work with a sense of responsibility and determination.
On the same day, I was told we would be off to a week-long staff retreat in a few days. It was a perfect opportunity for me to interact with everyone at CEHURD, hear about their work in the field, and learn about what CEHURD has done and aims to do in the next ten years. I am so grateful for the warm and welcoming environment I was surrounded with at the staff retreat, and for everyone who taught me how to dance the whole night on the last day of the retreat.
The tight-knit bonds among the staff members go beyond the organization. In one of the stakeholder meetings with healthcare workers I attended as part of the Strategic Litigation (SL) Programme, some of the team members repeatedly emphasized that we are here to learn from healthcare workers on the ground because they face various challenges on a daily basis which we aim to tackle. To ensure we receive insights from every participant in the meeting, papers were distributed and later collected by the team for reference.
Providing legal support for vulnerable populations is unarguably one of CEHURD’s strengths. Yet I realized that the quality of their services is also made possible by the strong bonds of trust with stakeholders including healthcare workers, local authorities, police officers, community health advocates, and others.
Other than attending meetings with stakeholders, my duties at the SL included drafting reports, research papers, and opinion responses to judgments. Through these activities, I got to learn in-depth about how the concepts of equality, discrimination, and rights of women and children are defined in the Constitution of Uganda and how cases of defilement and sexual violence are categorized in a way that undermines the welfare of certain groups of people, particularly adolescent girls above 14, under the current Penal Code Act.
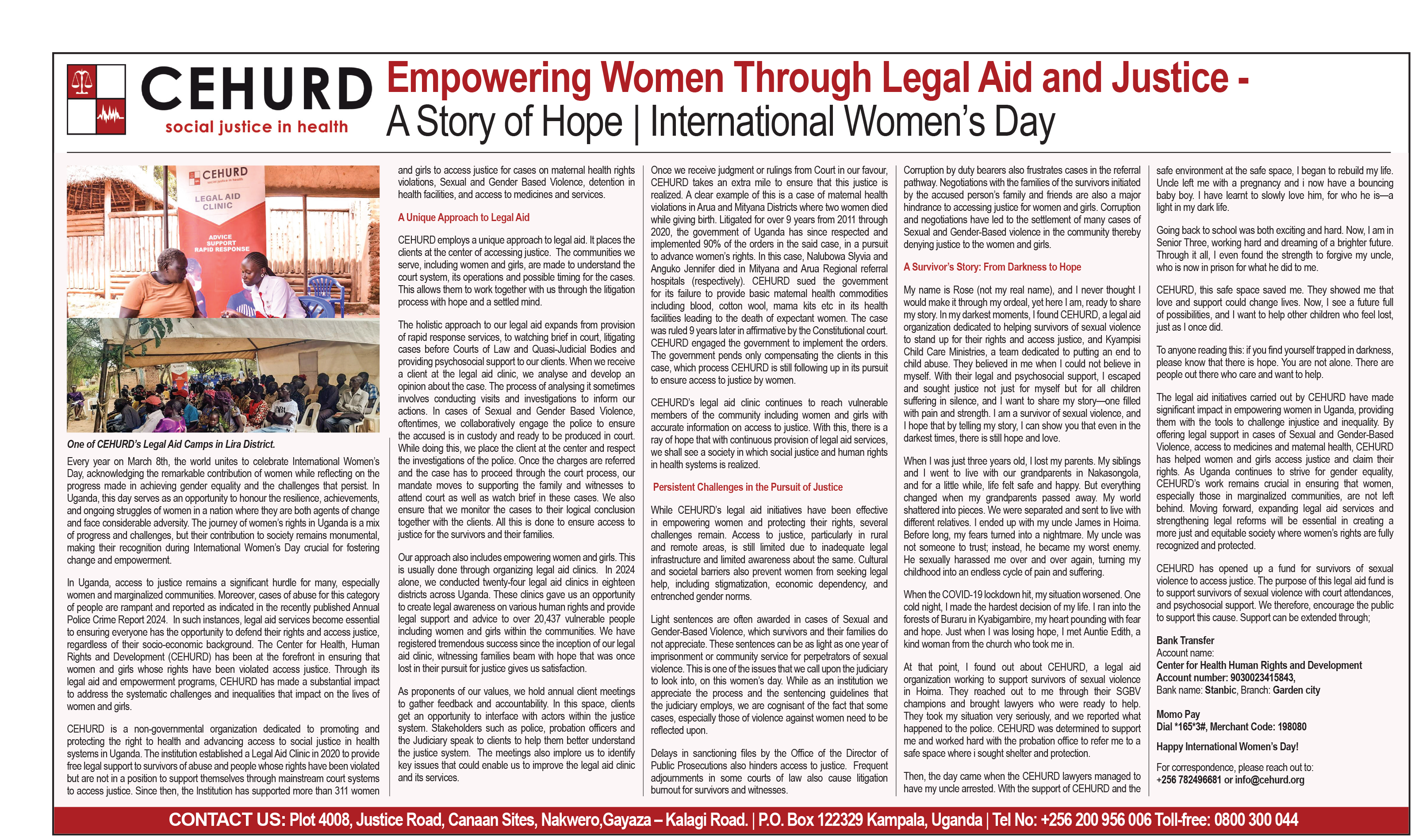
I spent my last two weeks at the Community Empowerment Programme (CEP). The highlight of my time at the CEP is a week-long field trip to one of the districts in Uganda to take part in legal aid clinics and a meeting with district stakeholders. It was full of learning experiences, as I got to delve into the gender- and health-related challenges through the interactions and discussions with community members, stakeholders, and the CEHURD team. The experience underscored the critical role of legal aid clinics and community sensitizations in raising awareness of health and human rights within communities, as they may not know about their rights and find legal services unaffordable and/or inaccessible, according to some of the team members. The conversations with stakeholders and the team shed light on the common issues faced by women and girls in the communities, such as gender-based violence, intimate partner violence, barriers to education and health services, and harmful gender norms.
As someone with an economics background, I wish to touch briefly upon what I witnessed from an economic perspective. Although I discussed them in greater detail in my other post, I explored the economic aspects of the health vulnerabilities among women and girls through field observations, discussions with the team, and relevant literature. One thing that stood out to me is the deep-rooted gender norms, and how they can increase their vulnerabilities through myriad channels. For example, discussions with some of the team members revealed how women may have little control over economic activities, which can confine them in abusive relationships and put them at a higher risk of intimate partner violence. Some issues, such as extra fees illegally charged by healthcare workers and/or police officers and barriers to education among pregnant girls, repeatedly emerged in discussions and meetings with stakeholders. Based on general observations in the field and the conversations with the team and stakeholders, I came to realize that these socioeconomic issues above may not only exacerbate the risk of gender-based violence but also keep the survivors away from reporting and/or seeking treatment.
Throughout my time at CEHURD, I witnessed both the innovative ideas and relentless effort poured into community-based projects and the difficulty sustaining them in the long run. The reasons can range from political and economic situations to the constant need of funds, and they were especially evident following the recent executive and legal actions on foreign aid from the US. Some of the team members revealed the uncertainty around the long-term sustainability of some of their impactful programs. I have heard of and seen organizations that struggle with similar issues of locally driven programs. I sincerely hope their commitment and determination to address structural injustices will be widely recognized and appreciated in and outside the country.
So far, I have gone over my learning experiences at CEHURD. Yet, I cannot wrap it up without mentioning what I miss the most as I write this essay: the people. From the first day to the last day, everyone at CEHURD offered me the most welcoming and warmest environment I could ever ask for. Starting every single day with greetings in Luganda and a cup of African tea made me feel like I had been there for a long time. The list of memorable things goes on, from being splashed with water by a water truck while on boda and laughing about it together, singing a notorious Valentine’s song (if you know, you know), to cutting a cake with my name on it together on my last day. No words can fully express how grateful I am to everyone at CEHURD for their support, warmth, and passion for ‘equitable health and human rights for all’ that made my time at CEHURD invaluable. I would also like to extend my sincere gratitude to Dr. Miya, Betty, and Edith from The AIDS Support Organization (TASO) Uganda for connecting me with this amazing organization. My experience would not have been possible without the foundation I gained through the research experience at TASO and your continuous support after the program.
Shiena Serikawa is a recent graduate from the University of British Columbia, Canada, with an interest in women’s economic empowerment. She has also been an intern at the Center for Health, Human Rights and Development (CEHURD).