By Shiena Serikawa, edited by CEHURD
My name is Shiena Serikawa, a recent graduate from the University of British Columbia, Canada with an interest in women’s economic empowerment. I had an opportunity to intern at the Center for Health, Human Rights and Development (CEHURD), where I visited communities in Namutumba District in Eastern Uganda. I was intrigued to explore the barriers to health among vulnerable communities to achieve ‘equitable health and human rights for all’ as CEHURD’s goal states, which resonates with my personal thoughts about health as a human right. My visit to the community, discussions with stakeholders, and review of relevant literature allowed me to understand the multidimensional socioeconomic factors that affect women’s health, notably harmful gender norms along with women’s economic disempowerment.
One of the major health concerns in Uganda is HIV/AIDS. As of 2023, approximately 1,500,000 adults and children were living with HIV in the country, of which around 60% consisted of women and girls aged 15 and above.[1] While HIV/AIDS has usually been associated with poverty, recent studies show that it is a disease of inequality due to its intricate connections with socioeconomic vulnerabilities and dependency that compel people in poverty, especially women, to make certain choices around sexual behaviour.[2][3]
One such factor is education. Schools are considered a crucial space for youth to gain sexual and reproductive health education, thereby reducing the risk of getting HIV and other sexually transmitted infections (STIs) for girls.[4][5] One study in South Africa found that young women aged 15-24 years without high school education had a higher prevalence of HIV than those with high school education, suggesting that education may prevent girls from getting HIV.[6] Yet, educational opportunities for boys are often prioritized over girls under economic hardships, as girls are expected to take care of households.[7][8] Girls may drop out of school for other reasons, such as a lack of sanitation facilities or early pregnancy.[9] Combined with the well-established association of education with employment opportunities, these findings suggest that girls who drop out of school for various reasons may face a higher risk of HIV infections and dependency.[10]
Moreover, a qualitative study in rural South-West Uganda showed that young women and girls, especially those who drop out of school, may engage in transactional sex with older men in exchange for money or material goods, which reinforces their economic dependency on men.[11] Young women may not have much say over sexual behaviour in such relationships, further escalating the risk of getting HIV and other STIs.[12]
Women’s agencies are limited not only in sexual interactions but also within households, which can lead to intimate partner violence (IPV) or gender-based violence (GBV). Violence against women is widespread in Uganda, as it has been considered an acceptable method to resolve conflicts within households.[13] Given that husbands are the primary decision-makers within households in Uganda, women have little power over household decisions.[14][15]
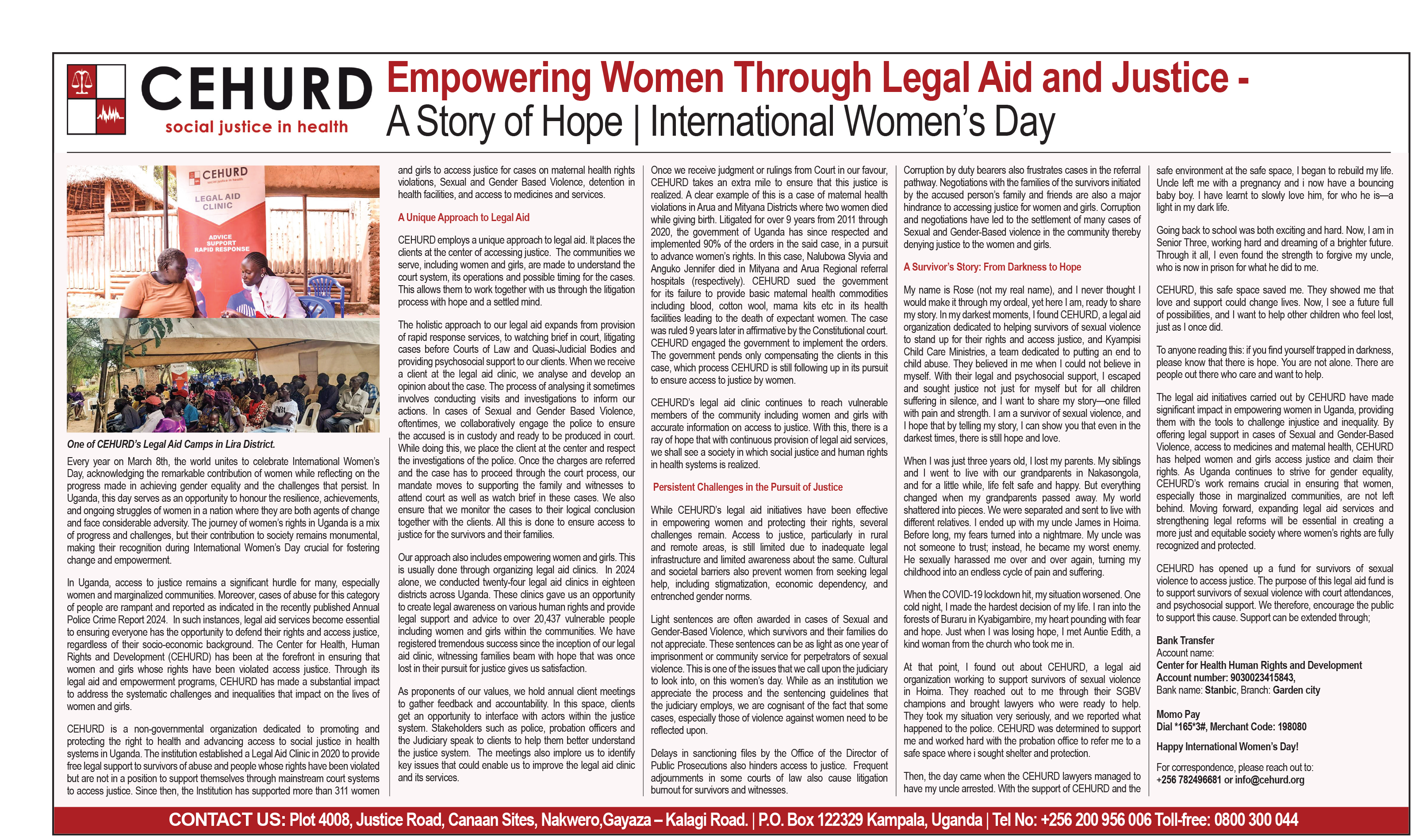
During my internship, I attended legal aid clinics conducted by CEHURD. The topics brought up included domestic violence and issues with their husbands not providing for their families, underlining harmful gender norms and women’s economic dependency on men. What is worse, even if they report their husbands for committing IPV, they may not be able to support themselves and their kids economically. According to Francis Serunjogi, the Manager of the Community Empowerment Department at CEHURD, some women stay in abusive relationships because they cannot provide for themselves and their families. Reporting spouses may not only exacerbate IPV but also generate stigma within their communities.
A study also found a critical role that household economic stress may play in the prevalence of IPV; household wealth and educational attainment of both partners were negatively correlated with reported IPV in Sub-Saharan Africa.[16] Yet, the relationship between IPV and women’s economic status is not clear-cut. The same study shed light on women’s relative economic empowerment, which found that when only women worked or earned more than men, IPV increased significantly.[17] Another study showed similar results; women’s economic status, such as their employment and earnings, was associated with an increase in spousal violence in Sub-Saharan Africa.[18] These findings suggest that economically empowered women were considered a threat if their male partners did not enjoy the same opportunities, highlighting the deeply entrenched gender norms.[19][20]
The evidence reveals that women’s health vulnerabilities consist of multiple socioeconomic factors that are intricately intertwined.[21][22] Such factors include but are not limited to poverty, education, and gender norms, which contribute to women’s economic dependency on men.[23]
Barriers to Health Services
A study found that 61.5% of women face barriers to health services in Sub-Saharan Africa.[24] Primary barriers include lack of money and distance to healthcare facilities, making general and maternal healthcare services less accessible for women.[25][26][27][28]
Lack of education may also prevent women from accessing healthcare. A study in Sub-Saharan Africa revealed that women with no or little formal education faced more barriers to healthcare services.[29] Other studies also identified women’s education as one of the determinants of the utilization of general and maternal healthcare.[30][31][32] A study in Malawi found that the negative association between the distance to health facilities and the utilization of maternal healthcare became stronger for women with limited health knowledge.[33] Educated women are more aware of the importance of healthcare, allowing them to make informed decisions.[34][35][36] Educational attainment may also determine their employment, which can affect their ability to afford healthcare.[37]
Women’s economic contributions to households may shape their access to healthcare. A study in Tanzania found that women’s contribution to household incomes was associated with an increase in the utilization of maternal healthcare services, suggesting that economically empowered women may use their income on their healthcare services without bargaining.[38] Yet in reality, women may not enjoy the benefits, given that male partners are the primary decision-makers and women have limited control over their health and well-being.[39][40][41]
Would economic empowerment alone reduce women’s health vulnerabilities?
Some interventions demonstrated a positive impact of women’s economic empowerment on health-related outcomes. A study in Malawi showed that cash transfer to female students aged 13-22 and their parents led to a reduction in the prevalence of HIV and risky sexual behaviour after 18 months.[42] Another study implemented a 5-year family-based economic empowerment intervention in Uganda, which improved HIV viral load suppression among adolescents of both genders aged 10-16.[43]
Yet, women’s economic dependency on men and its socioeconomic factors cannot be separated from the deeply entrenched gender norms. In Uganda, it is socially normalized for men to have decision-making power over household matters.[44][45] One qualitative study in Uganda revealed that, despite the positive impact of Village Savings and Loan Associations (VSLAs) on access to healthcare for children living with HIV, gender norms and men’s control over household decisions prevented some participants from attending activities.[46] Such social norms, along with the lack of accessible schools and household economic challenges, can hinder girls from going to school, further impeding their employment opportunities and economic independence.[47] We also discussed in the previous section the complex relationship between economic status and IPV—while greater household wealth was associated with an increase in IPV, women’s relative economic empowerment was associated with an increase in IPV.[48][49] The association of women’s relative economic empowerment with the prevalence of IPV can be derived from gender norms that do not appreciate women gaining power.[50][51]
It is evident that women’s health vulnerabilities and barriers to accessible healthcare are oftentimes driven by women’s economic dependency on men and deep-rooted gender norms that suppress women’s agencies. In fact, researchers emphasized gender inequalities caused by harmful gender norms as one of the structural factors of IPV, combined with other socioeconomic factors such as poverty, unemployment, and lack of economic activity.[52] Therefore, women’s economic empowerment interventions that incorporate gender-focused capacity building for both women and men may be crucial to eliminating health-related barriers.[53][54]
Although legal aid clinics run by CEHURD are not about economic empowerment, they help with gender-related matters from a legal perspective. Community sensitization provides a space for both women and men to learn about the fundamental human rights they deserve and realize any issues they face.
Women face unique health vulnerabilities and barriers to healthcare. Various socioeconomic factors are deeply interconnected and reinforce women’s economic dependency on men, which further fuels their vulnerabilities. Harmful gender norms that justify women’s subordination and gender-based violence against women are embedded in the communities in Uganda, accelerating their dependency and health vulnerabilities. Our discussion suggests that establishing healthcare services and facilities alone may not effectively address women’s access to healthcare. Approaches to the structural factors behind their vulnerabilities, such as gender-focused training for both women and men, may be necessary.
Ends.
Bibliography
African Development Bank Group. “Uganda Country Gender Profile.” African Development Bank. African Development Bank Group, February 2016. https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
Anik, Asibul Islam, Muhammad Ibrahim Ibne Towhid, and M Atiqul Haque. “Association of Spousal Violence and Women’s Empowerment Status among the Rural Women of Sub-Saharan Africa.” Journal of Biosocial Science 55, no. 1 (November 8, 2021): 55–73. https://doi.org/10.1017/s0021932021000602.
Aseweh Abor, Patience, Gordon Abekah‐Nkrumah, Kojo Sakyi, Charles K.D. Adjasi, and Joshua Abor. “The Socio‐Economic Determinants of Maternal Health Care Utilization in Ghana.” International Journal of Social Economics 38, no. 7 (June 7, 2011): 628–48. https://doi.org/10.1108/03068291111139258.
Bain, Luchuo Engelbert, Richard Gyan Aboagye, Robert Kokou Dowou, Eugene Justine Kongnyuy, Peter Memiah, and Hubert Amu. “Prevalence and Determinants of Maternal Healthcare Utilisation among Young Women in Sub-Saharan Africa: Cross-Sectional Analyses of Demographic and Health Survey Data.” BMC Public Health 22, no. 647 (April 5, 2022): 1–20. https://doi.org/10.1186/s12889-022-13037-8.
Baird, Sarah J., Richard S. Garfein, Craig T. McIntosh, and Berk Ozler. “Effect of a Cash Transfer Programme for Schooling on Prevalence of HIV and Herpes Simplex Type 2 in Malawi: A Cluster Randomised Trial.” Lancet 379 (April 7, 2012): 1320–29. https://doi.org/10.1016/S0140-6736(11)61709-1.
Kim, Julia, Paul Pronyk, Tony Barnett, and Charlotte Watts. “Exploring the Role of Economic Empowerment in HIV Prevention.” AIDS 22, no. Suppl 4 (December 2008): S57–71. https://doi.org/10.1097/01.aids.0000341777.78876.40.
McGuire, Finn, Noemi Kreif, and Peter C. Smith. “The Effect of Distance on Maternal Institutional Delivery Choice: Evidence from Malawi.” Health Economics 30 (June 6, 2021): 2144–67. https://doi.org/10.1002/hec.4368.
Nobelius, Ann-Maree, Bessie Kalina, Robert Pool, Jimmy Whitworth, Janice Chesters, and Robert Power. “Sexual Partner Types and Related Sexual Health Risk among Out-of-School Adolescents in Rural South-West Uganda.” AIDS Care 23, no. 2 (January 22, 2011): 252–59. https://doi.org/10.1080/09540121.2010.507736.
Pettifor, Audrey E, Brooke A Levandowski, Catherine MacPhail, Nancy S Padian, Myron S Cohen, and Helen V Rees. “Keep Them in School: The Importance of Education as a Protective Factor against HIV Infection among Young South African Women.” International Journal of Epidemiology 37, no. 6 (July 9, 2008): 1266–73. https://doi.org/10.1093/ije/dyn131.
Piot, Peter, Robert Greener, and Sarah Russell. “Squaring the Circle: AIDS, Poverty, and Human Development.” PLoS Medicine 4, no. 10 (October 23, 2007): 1571–75. https://doi.org/10.1371/journal.pmed.0040314.
Rujumba, Joseph, Carmen Roebersen, Susan Namara, Richard Ochen, Sharon Eva Ahumuza, Allen Tushabe, Mathias Akugizibwe, et al. “‘I No Longer Worry about Money for Transport to the Health Centre’ – Economic Empowerment of Caregivers of Children Living with HIV through Village Savings and Loan Associations: Experiences and Lessons from the ‘towards an AIDS Free Generation Program in Uganda (TAFU).’” BMC Health Services Research 25, no. 203 (February 4, 2025): 1–13. https://doi.org/10.1186/s12913-025-12303-w.
Seidu, Abdul-Aziz. “Mixed Effects Analysis of Factors Associated with Barriers to Accessing Healthcare among Women in Sub-Saharan Africa: Insights from Demographic and Health Surveys.” Edited by Yuka Kotozaki. PLOS ONE 15, no. 11 (November 9, 2020): 1–16. https://doi.org/10.1371/journal.pone.0241409.
Ssewamala, Fred M., Darejan Dvalishvili, Claude A. Mellins, Elvin H. Geng, Fredderick Makumbi, Torsten B. Neilands, Mary McKay, et al. “The Long-Term Effects of a Family Based Economic Empowerment Intervention (Suubi+Adherence) on Suppression of HIV Viral Loads among Adolescents Living with HIV in Southern Uganda: Findings from 5-Year Cluster Randomized Trial.” PLOS ONE 15, no. 2 (2020): 1–13. https://doi.org/10.1371/journal.pone.0228370.
Stöckl, Heidi, Anushé Hassan, Meghna Ranganathan, and Abigail M. Hatcher. “Economic Empowerment and Intimate Partner Violence: A Secondary Data Analysis of the Cross-Sectional Demographic Health Surveys in Sub-Saharan Africa.” BMC Women’s Health 21, no. 241 (June 12, 2021): 1–13. https://doi.org/10.1186/s12905-021-01363-9.
UNAIDS. “Uganda.” UNAIDS. UNAIDS, 2023. https://www.unaids.org/en/regionscountries/countries/uganda.
UNESCO. “Booklet 2: HIV & AIDS and Supportive Learning Environments. Good Policy and Practice in HIV & AIDS and Education (Booklet Series).” UNESCO Digital Library. Paris: UNESCO, 2008. https://unesdoc.unesco.org/ark:/48223/pf0000146122.
Westeneng, Judith, and Ben D’Exelle. “How Economic Empowerment Reduces Women’s Reproductive Health Vulnerability in Tanzania.” The Journal of Development Studies 51, no. 11 (September 2015): 1459–74. https://doi.org/10.1080/00220388.2015.1041514.
[1] UNAIDS, “Uganda,” UNAIDS (UNAIDS, 2023), https://www.unaids.org/en/regionscountries/countries/uganda.
[2] Julia Kim et al., “Exploring the role of economic empowerment in HIV prevention,” AIDS 22, no. Suppl 4 (December 2008): S57-61, https://doi.org/10.1097/01.aids.0000341777.78876.40.
[3] Peter Piot, Robert Greener, and Sarah Russell, “Squaring the circle: AIDS, poverty, and human development,” PLoS Medicine 4, no. 10 (October 23, 2007): 1571, https://doi.org/10.1371/journal.pmed.0040314.
[4] UNESCO, “Booklet 2: HIV & AIDS and supportive learning environments. Good policy and practice in HIV & AIDS and education (Booklet Series),” UNESCO Digital Library (Paris: UNESCO, 2008): 30, https://unesdoc.unesco.org/ark:/48223/pf0000146122.
[5] Audrey E Pettifor et al., “Keep them in school: The importance of education as a protective factor against HIV infection among young South African women,” International Journal of Epidemiology 37, no. 6 (July 9, 2008): 1269, https://doi.org/10.1093/ije/dyn131.
[6] Ibid.
[7] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 5, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[8] Audrey E Pettifor et al., “Keep them in school: The importance of education as a protective factor against HIV infection among young South African women,” International Journal of Epidemiology 37, no. 6 (July 9, 2008): 1270, https://doi.org/10.1093/ije/dyn131.
[9] UNESCO, “Booklet 2: HIV & AIDS and supportive learning environments. Good policy and practice in HIV & AIDS and education (Booklet Series),” UNESCO Digital Library (Paris: UNESCO, 2008): 22, https://unesdoc.unesco.org/ark:/48223/pf0000146122.
[10] Ibid.
[11] Ann-Maree Nobelius et al., “Sexual partner types and related sexual health risk among out-of-school adolescents in rural South-West Uganda,” AIDS Care 23, no. 2 (January 22, 2011): 257, https://doi.org/10.1080/09540121.2010.507736.
[12] Ibid.
[13] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 11, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[14] Ibid.
[15] Joseph Rujumba et al., “‘I no longer worry about money for transport to the health centre’ – economic empowerment of caregivers of children living with HIV through Village Savings and Loan Associations: Experiences and lessons from the ‘Towards an AIDS Free Generation Program in Uganda (TAFU),’” BMC Health Services Research 25, no. 203 (February 4, 2025): 9, https://doi.org/10.1186/s12913-025-12303-w.
[16] Heidi Stöckl et al., “Economic empowerment and intimate partner violence: A secondary data analysis of the cross-sectional Demographic Health Surveys in Sub-Saharan Africa,” BMC Women’s Health 21, no. 241 (June 12, 2021): 4-7, https://doi.org/10.1186/s12905-021-01363-9.
[17] Ibid., 5.
[18] Asibul Islam Anik, Muhammad Ibrahim Ibne Towhid, and M Atiqul Haque, “Association of spousal violence and women’s empowerment status among the rural women of Sub-Saharan Africa,” Journal of Biosocial Science 55, no. 1 (November 8, 2021): 64, 68, https://doi.org/10.1017/s0021932021000602.
[19] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 16, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[20] Heidi Stöckl et al., “Economic empowerment and intimate partner violence: A secondary data analysis of the cross-sectional Demographic Health Surveys in Sub-Saharan Africa,” BMC Women’s Health 21, no. 241 (June 12, 2021): 7, 12, https://doi.org/10.1186/s12905-021-01363-9.
[21] Julia Kim et al., “Exploring the role of economic empowerment in HIV prevention,” AIDS 22, no. Suppl 4 (December 2008): S57-61, https://doi.org/10.1097/01.aids.0000341777.78876.40.
[22] Peter Piot, Robert Greener, and Sarah Russell, “Squaring the circle: AIDS, poverty, and human development,” PLoS Medicine 4, no. 10 (October 23, 2007): 1571, https://doi.org/10.1371/journal.pmed.0040314.
[23] Ibid.
[24] Abdul-Aziz Seidu, “Mixed effects analysis of factors associated with barriers to accessing healthcare among women in Sub-Saharan Africa: Insights from Demographic and Health Surveys,” ed. Yuka Kotozaki, PLOS ONE 15, no. 11 (November 9, 2020): 9, https://doi.org/10.1371/journal.pone.0241409.
[25] Patience Aseweh Abor et al., “The socio‐economic determinants of maternal health care utilization in Ghana,” International Journal of Social Economics 38, no. 7 (June 7, 2011): 643-645, https://doi.org/10.1108/03068291111139258.
[26] Luchuo Engelbert Bain et al., “Prevalence and determinants of maternal healthcare utilisation among young women in Sub-Saharan Africa: Cross-sectional analyses of Demographic and Health Survey data,” BMC Public Health 22, no. 647 (April 5, 2022): 5, https://doi.org/10.1186/s12889-022-13037-8.
[27] Finn McGuire, Noemi Kreif, and Peter C. Smith, “The effect of distance on maternal institutional delivery choice: Evidence from Malawi,” Health Economics 30 (June 6, 2021): 2158, https://doi.org/10.1002/hec.4368.
[28] Abdul-Aziz Seidu, “Mixed effects analysis of factors associated with barriers to accessing healthcare among women in Sub-Saharan Africa: Insights from Demographic and Health Surveys,” ed. Yuka Kotozaki, PLOS ONE 15, no. 11 (November 9, 2020): 11-13, https://doi.org/10.1371/journal.pone.0241409.
[29] Ibid., 12.
[30] Patience Aseweh Abor et al., “The socio‐economic determinants of maternal health care utilization in Ghana,” International Journal of Social Economics 38, no. 7 (June 7, 2011): 642, https://doi.org/10.1108/03068291111139258.
[31] Luchuo Engelbert Bain et al., “Prevalence and determinants of maternal healthcare utilisation among young women in Sub-Saharan Africa: Cross-sectional analyses of Demographic and Health Survey data,” BMC Public Health 22, no. 647 (April 5, 2022): 5, https://doi.org/10.1186/s12889-022-13037-8.
[32] Abdul-Aziz Seidu, “Mixed effects analysis of factors associated with barriers to accessing healthcare among women in Sub-Saharan Africa: Insights from Demographic and Health Surveys,” ed. Yuka Kotozaki, PLOS ONE 15, no. 11 (November 9, 2020): 12, https://doi.org/10.1371/journal.pone.0241409.
[33] Finn McGuire, Noemi Kreif, and Peter C. Smith, “The effect of distance on maternal institutional delivery choice: Evidence from Malawi,” Health Economics 30 (June 6, 2021): 2158, https://doi.org/10.1002/hec.4368.
[34] Patience Aseweh Abor et al., “The socio‐economic determinants of maternal health care utilization in Ghana,” International Journal of Social Economics 38, no. 7 (June 7, 2011): 642, https://doi.org/10.1108/03068291111139258.
[35] Luchuo Engelbert Bain et al., “Prevalence and determinants of maternal healthcare utilisation among young women in Sub-Saharan Africa: Cross-sectional analyses of Demographic and Health Survey data,” BMC Public Health 22, no. 647 (April 5, 2022): 9, https://doi.org/10.1186/s12889-022-13037-8.
[36] Abdul-Aziz Seidu, “Mixed effects analysis of factors associated with barriers to accessing healthcare among women in Sub-Saharan Africa: Insights from Demographic and Health Surveys,” ed. Yuka Kotozaki, PLOS ONE 15, no. 11 (November 9, 2020): 12, https://doi.org/10.1371/journal.pone.0241409.
[37] Ibid.
[38] Judith Westeneng and Ben D’Exelle, “How economic empowerment reduces women’s reproductive health vulnerability in Tanzania,” The Journal of Development Studies 51, no. 11 (September 2015): 1471, https://doi.org/10.1080/00220388.2015.1041514.
[39] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 11, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[40] Joseph Rujumba et al., “‘I no longer worry about money for transport to the health centre’ – economic empowerment of caregivers of children living with HIV through Village Savings and Loan Associations: Experiences and lessons from the ‘Towards an AIDS Free Generation Program in Uganda (TAFU),’” BMC Health Services Research 25, no. 203 (February 4, 2025): 9, https://doi.org/10.1186/s12913-025-12303-w.
[41] Judith Westeneng and Ben D’Exelle, “How economic empowerment reduces women’s reproductive health vulnerability in Tanzania,” The Journal of Development Studies 51, no. 11 (September 2015): 1459, https://doi.org/10.1080/00220388.2015.1041514.
[42] Sarah J. Baird et al., “Effect of a cash transfer programme for schooling on prevalence of HIV and Herpes Simplex Type 2 in Malawi: A cluster randomised trial,” Lancet 379 (April 7, 2012): 1327-28, https://doi.org/10.1016/S0140-6736(11)61709-1.
[43] Fred M. Ssewamala et al., “The long-term effects of a family based economic empowerment intervention (Suubi+Adherence) on suppression of HIV viral loads among adolescents living with HIV in southern Uganda: Findings from 5-year cluster randomized trial,” PLOS ONE 15, no. 2 (2020): 8-10, https://doi.org/10.1371/journal.pone.0228370.
[44] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 11, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[45] Joseph Rujumba et al., “‘I no longer worry about money for transport to the health centre’ – economic empowerment of caregivers of children living with HIV through Village Savings and Loan Associations: Experiences and lessons from the ‘Towards an AIDS Free Generation Program in Uganda (TAFU),’” BMC Health Services Research 25, no. 203 (February 4, 2025): 9, https://doi.org/10.1186/s12913-025-12303-w.
[46] Ibid.
[47] Audrey E Pettifor et al., “Keep them in school: The importance of education as a protective factor against HIV infection among young South African women,” International Journal of Epidemiology 37, no. 6 (July 9, 2008): 1271, https://doi.org/10.1093/ije/dyn131.
[48] Asibul Islam Anik, Muhammad Ibrahim Ibne Towhid, and M Atiqul Haque, “Association of spousal violence and women’s empowerment status among the rural women of Sub-Saharan Africa,” Journal of Biosocial Science 55, no. 1 (November 8, 2021): 69, https://doi.org/10.1017/s0021932021000602.
[49] Heidi Stöckl et al., “Economic empowerment and intimate partner violence: A secondary data analysis of the cross-sectional Demographic Health Surveys in Sub-Saharan Africa,” BMC Women’s Health 21, no. 241 (June 12, 2021): 5, https://doi.org/10.1186/s12905-021-01363-9.
[50] African Development Bank Group, “Uganda country gender profile,” African Development Bank (African Development Bank Group, February 2016): 16, https://www.afdb.org/fileadmin/uploads/afdb/Documents/Project-and-Operations/UGANDA_COUNTRY_GENDER_PROFILE-2016.pdf.
[51] Heidi Stöckl et al., “Economic empowerment and intimate partner violence: A secondary data analysis of the cross-sectional Demographic Health Surveys in Sub-Saharan Africa,” BMC Women’s Health 21, no. 241 (June 12, 2021): 7, 12, https://doi.org/10.1186/s12905-021-01363-9.
[52] Ibid., 2.
[53] Julia Kim et al., “Exploring the role of economic empowerment in HIV prevention,” AIDS 22, no. Suppl 4 (December 2008): S61, https://doi.org/10.1097/01.aids.0000341777.78876.40.
[54] Heidi Stöckl et al., “Economic empowerment and intimate partner violence: A secondary data analysis of the cross-sectional Demographic Health Surveys in Sub-Saharan Africa,” BMC Women’s Health 21, no. 241 (June 12, 2021): 12, https://doi.org/10.1186/s12905-021-01363-9.