By Denis Juuko
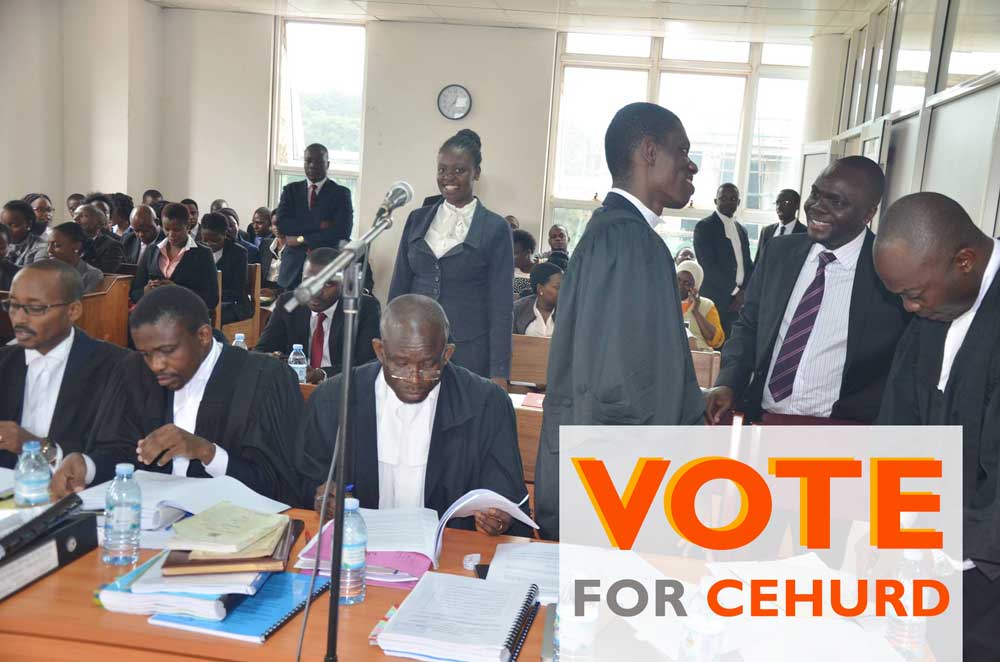
In collaboration with Ipas- Africa Alliance, CEHURD held a workshop for law enforcement institutions on the legal and policy environment for access to safe abortion services in Uganda.
The workshop built synergies between law enforcement officers and health workers in dealing with the unwarranted arrests, detention, and prosecution of women, girls, and healthcare providers for offering abortion related services.
At the workshop, participants shared their experiences of how they deal with issues related abortion in the communities they serve.
It was noted that post abortion care is not restricted but police is not aware about the position of the law hence resulting to unwarranted arrests, embarrassments and harassment of health practitioners who offer post-abortion care, which leads to stigma in the communities where they operate.
Health workers during the discussions brought to the attention of law enforcement officers that some women and girls come with inevitable abortions and therefore the law enforcement officers need to understand the situations the women are in. They equally emphasized the need to respect their professions since they take oaths of saving lives at all costs.
As a take home for the participants, it was agreed that law enforcement officers and health workers need to have a good working relationship to save the lives of women who suffer complications and death as a result of clandestine unsafe abortions.